Choosing a PDT laser is complex. The wrong one can ruin your device's performance and budget. The key is understanding the system-level trade-offs for a successful design.
The right PDT laser isn't just about wavelength. It's a balance between the photosensitizer's absorption peak, required tissue penetration, and device-level needs like power stability, costo, y gestión térmica. A holistic, system-level approach is crucial for a reliable and effective medical device.
I remember a conversation with a new client a few years ago. They were a promising medical device startup, and they were very focused on one thing: getting a laser at a very specific, non-standard wavelength. They believed this was their unique selling point. We spent weeks discussing the technical challenges and supply chain risks. This experience highlighted a common issue I see all the time. Engineers and product managers often focus intensely on one parameter, like wavelength, without fully appreciating how it connects to the entire system. Before you can select the right laser, you have to understand the fundamental process it drives. So, let's start with the basics.
How Does PDT Use Light and a Photosensitizer for Selective Cell Destruction?
You know PDT involves light, but do you grasp the core mechanism? Misunderstanding it can lead to bad design choices. Let's quickly review the fundamentals for better device development.
PDT works by using a specific wavelength of light to activate a photosensitizer drug. This drug, when activated, produces a reactive form of oxygen that selectively destroys nearby targeted cells, like tumors or bacteria, while minimizing damage to surrounding healthy tissue.
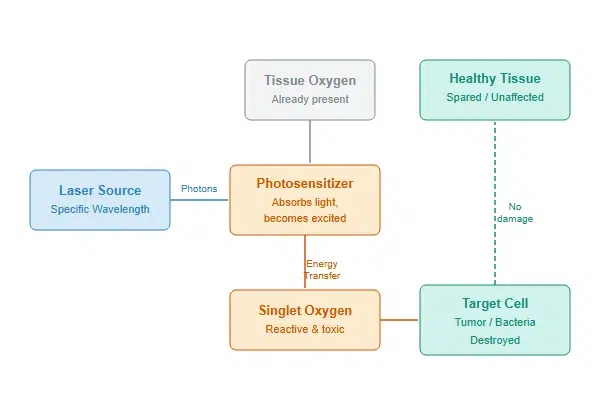
From my perspective as a laser manufacturer, the entire process is a fascinating interplay of biology and physics. Your device design needs to respect both. The process depends on three key components: the photosensitizer drug, oxygen already present in the tissue, and the light source, which is our laser. The photosensitizer is designed to accumulate in specific target cells.1 It stays inactive until we shine a light on it. Our laser module’s job is to deliver photons of a very specific energy level (longitud de onda) to that exact spot. When the photosensitizer absorbs these photons, it transfers that energy to oxygen molecules in the cell, creating something called singlet oxygen. This is a highly reactive form of oxygen that is toxic to the cell, causing it to die. It's a clean and localized process. Our responsibility is to provide the perfect "on switch" in the form of a stable, reliable laser.
The Three Pillars of PDT
| Component | Role in Therapy | Your Design Consideration |
|---|---|---|
| Photosensitizer | Accumulates in target cells; determines the required wavelength. | Your laser's wavelength must precisely match the drug's absorption peak. |
| Oxygen | Becomes reactive (singlet oxygen) to destroy the cell. | Assumed to be present in the target tissue. |
| Light Source (Láser) | Activates the photosensitizer with photons of a specific energy. | Your laser must deliver the correct wavelength, fuerza, and dose reliably. |
What Wavelengths like 630nm, 665Nuevo Méjico, and 850nm are Needed for Different Photosensitizers?
You see common PDT wavelengths like 630nm, but why those specific numbers? Choosing a wavelength blindly is risky. The answer lies in the photosensitizer's absorption and tissue optics.
Wavelengths like 630nm and 665nm are chosen because they match the absorption peaks of common photosensitizers (like porphyrins) and penetrate tissue well. Higher wavelengths like 850nm are used for deeper targets, matching newer sensitizers designed for the "therapeutic window" of tissue.
The most common question I get is, "Do you have a laser at exactly 652nm?" While we can often build one, it's not always the right question to start with. The ideal wavelength is a function of two competing factors: the photosensitizer's absorption peak and the light's penetration depth in tissue. Most first-generation photosensitizers have strong absorption peaks in the red light spectrum, around 630-670nm. This range also happens to fall within the "therapeutic window" of tissue (roughly 600-1100nm), where light penetration is maximized because absorption by water and hemoglobin is lower. So, red light offers a good balance. Newer photosensitizers are being designed to absorb light at longer wavelengths, like 850nm, to treat deeper tumors. From a manufacturer's standpoint, there are also practical trade-offs. Diodes for common wavelengths like 635nm or 660nm are mature, confiable, and cost-effective. A highly specific custom wavelength might use a less common diode, which can impact cost, lead times, and long-term supply stability.
Wavelength Selection Factors
| Factor | Descripción | Implication for Device Integrators |
|---|---|---|
| Absorption Peak | The wavelength at which the photosensitizer is most efficiently activated. | You must match your laser wavelength to this peak for maximum efficacy. |
| Tissue Penetration | Longer wavelengths generally penetrate deeper into biological tissue. | For deeper targets, you need a longer wavelength and a photosensitizer that matches. |
| Diode Availability | The maturity and availability of the semiconductor laser diode at that wavelength. | Common wavelengths are cheaper, more reliable, and have a more stable supply chain. |
How Does Fiber Delivery Differ for Endoscopic vs. Surface PDT Applications?
Your laser is ready, but how do you deliver the light precisely? A bad delivery system can ruin the treatment. Fiber optics are the solution, but they must be tailored for different applications.
For endoscopic PDT, light is delivered via thin, flexible optical fibers through the body's channels to internal targets. For surface treatments, light is often delivered using larger fibers with microlens arrays or diffusers to illuminate a wide, uniform area on the skin.

When a customer comes to us for a fiber-coupled laser module, my first question is always about the application. The design of the module's output is completely different for these two scenarios. For endoscopic applications, the challenge is coupling high optical power into a very thin and flexible fiber, sometimes with a core diameter as small as 200 or 400 microns. This requires precise optical alignment inside the laser module and a robust, reliable fiber connector like an SMA 905. The numerical aperture (N / A) of the fiber is also critical, as it determines how the light will exit the fiber tip and illuminate the tissue. For surface treatments, the goal is different. Here, we need to illuminate a larger area, perhaps several square centimeters, with a very uniform power density. A single "hot spot" is unacceptable. This often involves using a larger core fiber that feeds into a custom handpiece with homogenizing optics, like microlens arrays or engineered diffusers. The laser module itself might be the same, but the delivery system it's designed to work with dictates many of its output characteristics.
Fiber Delivery Design Comparison
| Parámetro | Endoscopic PDT | Surface PDT |
|---|---|---|
| Objetivo | Internal organs, tumors | Skin, surface lesions |
| Fiber Type | Thin, flexible, small core (P.EJ., 400µm) | Often larger core, feeding a diffuser |
| Key Challenge | High coupling efficiency into a small fiber | Achieving uniform power density over a large area |
| Module Focus | Precise alignment, robust connector (SMA) | Stable power output, compatibility with homogenizing optics |
How Do You Determine Power and Fluence Requirements for Clinical PDT Protocols?
Delivering the right "dose" of light is critical. Get it wrong, and the treatment fails or causes harm. You need to master power, fluence, and fluence rate to design a safe device.
Fuerza (Watts) is the rate of energy delivery. Fluence (Joules/cm²) is the total energy delivered per unit area. These are determined by clinical protocols for a specific photosensitizer and condition. The laser must provide stable power over time to deliver the required fluence accurately.

From a component manufacturer's perspective, this is where laser stability becomes the most critical parameter. Clinical protocols are built around a specific "dose" of light, which is called fluence. Let's break it down. Fuerza, measured in Watts (W.), is how fast the laser sends out energy. Fluence, measured in Joules per square centimeter (J/cm²), is the total amount of energy delivered to a specific area. These are related by time: delivering 1 Watt of power for 1 second gives you 1 Joule of energy. If the clinical protocol calls for 100 J/cm², your device software will calculate the required treatment time based on the laser's power output and the spot size. But here's the catch: that calculation assumes the laser's power is perfectly stable. If your laser's output power drops by 15% during a 10-minute procedure because it's overheating, you have under-dosed the patient by 15%. This is why simply looking at a datasheet that says "5W output" is not enough. We perform rigorous long-term aging and stability tests to ensure our modules can maintain their specified power under real-world operating conditions.
What's the Best Way for an OEM to Select a Laser Diode Module for a PDT Device?
Choosing a laser module for your OEM device is daunting. Focusing on one spec, like wavelength, can cause huge integration problems. A system-level approach is your best bet for success.
OEMs should select a laser module by providing the manufacturer with system-level requirements, not just a wavelength. Specify the photosensitizer, target depth, required power stability, thermal constraints, and desired lifespan. This allows the laser supplier to recommend or design a fully optimized and reliable solution.

I want to reframe how you approach buying a laser module. Instead of starting the conversation with a part number, start it with your problem. When you treat us as a partner instead of just a component vendor, we can help you de-risk your entire project. A good laser manufacturer has seen dozens of integration projects and understands the hidden pitfalls. We know which diodes have the most stable supply chains, the thermal management challenges associated with certain power levels, and the best optical designs for specific fiber types. By sharing your system-level requirements, you allow us to bring that experience to your project. This collaborative approach moves the conversation from a simple transaction to a co-design process, which almost always results in a better, more reliable, and more commercially viable final product.
How to Talk to Your Laser Supplier
| Instead of Asking This... | Ask This Instead... |
|---|---|
| "Do you have a 5W, 665nm laser?" | "We need to deliver 150 J/cm² over a 2cm² area, activating Photosensitizer X. What module provides the most stable power with our cooling constraints?" |
| "What's the price for your 635nm module?" | "We are targeting a specific device cost and require a 20,000-hour lifespan. What 635nm module options balance cost, fiabilidad, and performance for this goal?" |
| "I need a laser with an SMA connector." | "Our device uses a 400µm, 0.22 NA fiber for an endoscopic application. What module will give us the highest and most stable coupling efficiency for this setup?" |
Conclusión
Choosing the right PDT laser is a system design challenge. By focusing on the photosensitizer, application, and key trade-offs with your supplier, you can build a more reliable device.
"Biochemical Basis of Selective Accumulation and Targeted Delivery ...", https://pubmed.ncbi.nlm.nih.gov/36509715/. A source can describe the mechanisms for preferential photosensitizer accumulation in malignant tissues, often attributed to the enhanced permeability and retention (EPR) effect, as well as specific cellular uptake pathways. Evidence role: mechanism; source type: paper. Supports: The mechanisms by which photosensitizers preferentially accumulate in target tissues, particularly tumors.. ↩